Retake
P8) Fever and foul smelling urine in a 6-month-old
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with dysuria.
- Review the DDx considerations in a pediatric patient with dysuria.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with dysuria.
History
A 6-month-old is brought into the clinic due to fever, cloudy, foul smelling urine, and irritability. She is up to date on her vaccinations and was born full-term by vaginal delivery without complications. There is no history of constipation.
Physical Exam
BP: 100/70, HR 135 bpm, RR 40 bpm, Temp 40.0 C, O2 saturation 99%.
Abdominal: suprapubic and costovertebral angle (CVA) tenderness.
Labs
UA: cloudy urine positive for nitrites and leukocyte esterase. 5 RBC/hpf. 10-20 WBC/hpf.
Provisional Diagnosis
Select the Dx you believe is most appropriate
This patient's history, symptoms, and lab results align with a UTI diagnosis. In a young child with a febrile UTI, vesicoureteral reflux (VUR), among other structural abnormalities, is a concern as it enables bacteria to access the usually sterile upper urinary tract, predisposing them to pyelonephritis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine, but expedited workup, as their condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
An ultrasound is a noninvasive and readily available imaging method that can detect underlying urinary tract anomalies, such as hydronephrosis, duplex renal system, hydroureter, and ureterocele. Although ultrasound has low sensitivity for detecting VUR and renal scarring, it is beneficial in identifying congenital renal anomalies after the first episode of a UTI.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
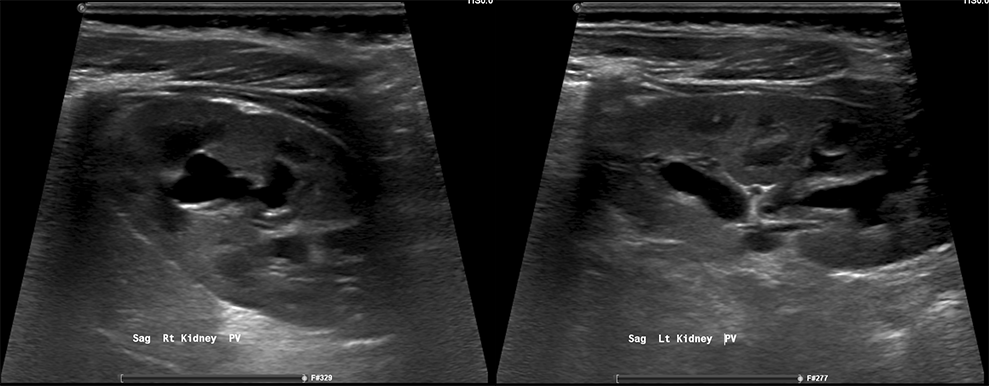
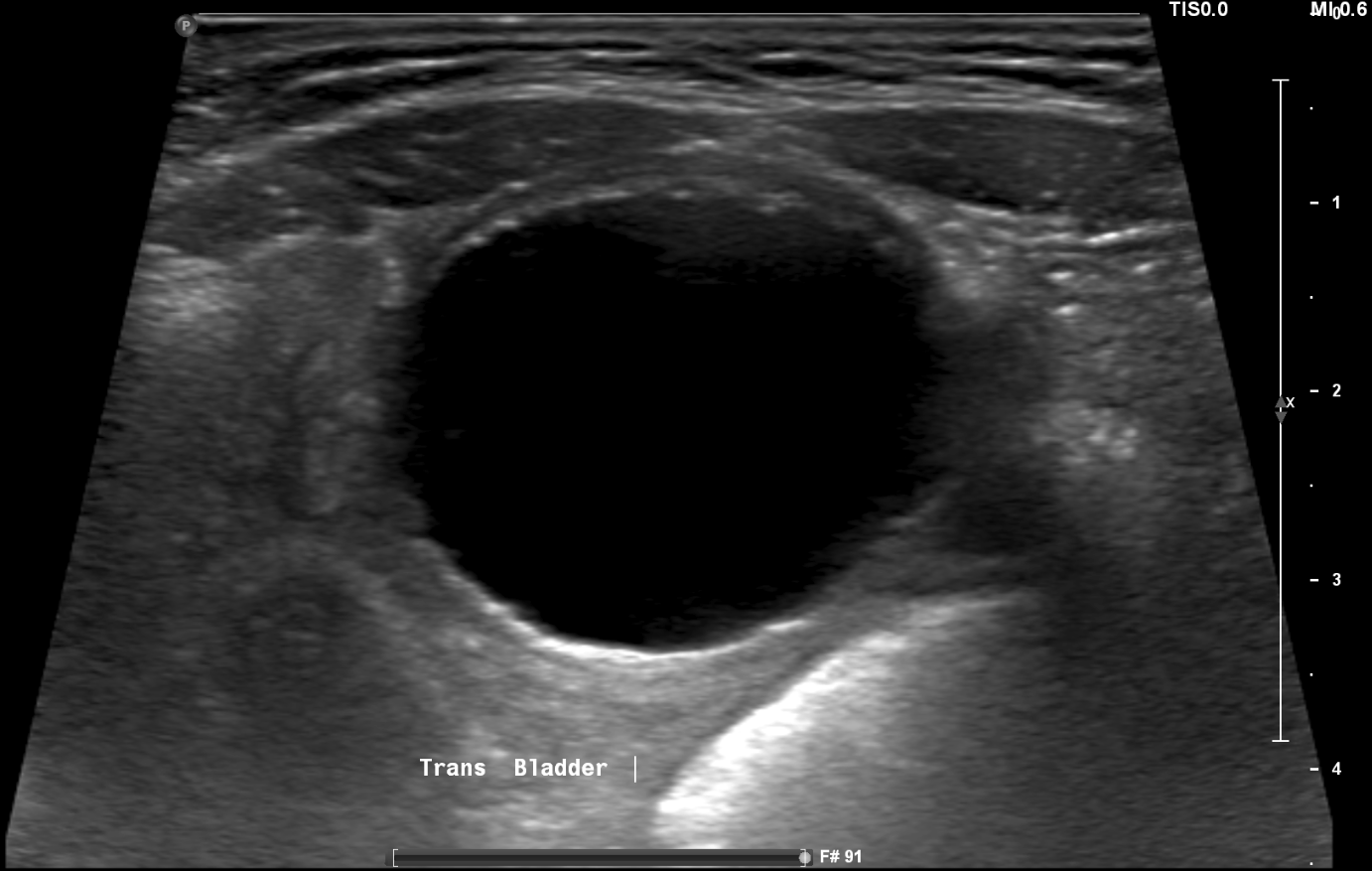
Ultrasound
The kidneys are normal.
There is bilateral hydronephrosis.
The bladder is normal.
There is no bladder wall thickening, diverticula, or masses.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A VCUG should be obtained to determine if VUR is the underlying cause of the hydronephrosis.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
VCUG
There is evidence of VUR.
VUR is present, indicating urine backflow from the bladder into the ureters and kidneys during voiding.
The VUR grade is at least:
Grade I VUR affects the ureter partially, while Grade II reaches the ureter and renal pelvis. Grade III results in mild-moderate dilation of the ureter and renal pelvis with some blunting of the calyces. Grade IV exhibits moderate-severe dilation and more calyceal blunting. Grade V leads to significant calyceal distortion and potential kidney damage. In this case, there is grade 4 left-sided and grade 3 right-sided VUR.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
None. The diagnosis is made with the VCUG.
What is your Diagnosis now that you have seen the imaging results?
Given that this UTI is secondary to VUR, which involves both structural and functional issues, it would be classified as complicated. In this case, it is likely primary VUR, resulting from a malfunctioning valve-like mechanism at the UVJ that allows urine backflow into the ureters and kidneys. The patient does not have any issues, such as bladder outlet obstruction, chronic constipation, or neurogenic bladder, that would suggest secondary VUR.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient’s condition is not immediately life-threatening. However, they require expedited workup.
Assessment and Plan
Please provide your assessment and plan for this patient
A 6-month-old patient presents with a febrile UTI. Workup includes a renal ultrasound, demonstrating hydronephrosis, and a VCUG revealing grade 4 left-sided and grade 3 right-sided VUR. The patient should be initiated on appropriate antibiotic therapy based on culture and sensitivity results, following empiric therapy, with outpatient follow-up to ensure resolution. The patient should be placed on antibiotic prophylaxis and referred to a pediatric urologist for further evaluation and management, including discussion of potential surgical or endoscopic interventions.
Lessons Learned:
- Structural and functional abnormalities, such as VUR, should be considered in infants or children presenting with febrile UTIs or recurrent UTIs.
- A routine ultrasound may be ordered as an initial imaging modality, detecting underlying urinary tract anomalies like hydronephrosis, duplex renal systems, hydroureters, and ureteroceles.
- A voiding cystourethrogram (VCUG) is the gold standard for diagnosing and grading VUR.
- Primary VUR arises due to a congenital abnormality in the ureterovesical junction (UVJ), where its valve-like mechanism fails to close properly during voiding, causing urine to flow back into the ureters and kidneys. This condition may resolve spontaneously as the child grows.
- Secondary VUR is caused by an acquired obstruction, such as bladder outlet obstruction (posterior urethral valve), neurogenic bladder, or chronic constipation.
- Treatment depends on the grade of the VUR. Surgical correction is often considered for those with persistent high-grade VUR beyond two or three years of age, those who fail medical therapy with breakthrough infections, those who have significant side effects from continuous prophylactic antibiotics, or those with noncompliance with a long-term medical regimen.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}